
For the autoimmune woman still doing Botox, fillers, or microneedling… read this before your next treatment
For the woman who has done the internal work and is ready for a more supportive, non‑fractional laser approach to improving fine lines, skin texture, and firmness – at home and without pain.
This publication contains affiliate links. If you make a purchase I will receive a commission. Your price remains the same. Thank you!
The Conversation Nobody Is Having in the Biohacking Space
You’ve spent years learning how your body works. You understand that skin health is downstream of nutrition. That collagen is protein-dependent. That inflammation ages you faster than sun exposure. That hormones, gut health, and cellular repair are all connected to what you see in the mirror.
You’ve done the internal work most people never even know exists. And yet. When it comes to external skin treatments, most women – even the most biologically literate ones – are still operating from a completely different framework. One that relies on controlled damage to get results.
Microneedling. Lasers. Chemical peels. Injectables. All of them work on the same basic principle: injure the tissue, trigger a repair response, hope the repair response produces more collagen than the damage cost you.
And here’s the question I’ve been sitting with: if you’ve spent years building a body that is primed to repair, produce collagen, and regenerate tissue… why are you still forcing it through damage to get there?
How We Got Here: The Damage-Based Paradigm
The modern aesthetic industry was built on a simple observation: when skin is injured, it heals. And sometimes, that healing produces improvements – smoother texture, firmer tissue, reduced scarring. So the industry built an entire treatment model around controlled injury. And for a long time, it was the best option available.
But here’s what that model doesn’t account for: the quality of your repair response determines the quality of your results. If your body is inflamed, nutrient-depleted, hormonally dysregulated, or immune-compromised – your repair response is compromised too.
This is why the same treatment produces dramatically different results in different women. It’s not the treatment. It’s the biological terrain it’s working with.
And for autoimmune women specifically, damage-based treatments carry an additional layer of complexity: inflammatory responses can be exaggerated and prolonged, healing timelines are less predictable, immune activation from injury can trigger systemic flares, repeated damage cycles can accelerate barrier breakdown over time.
You’ve worked too hard on your internal terrain to keep running it through a damage cycle.
What Collagen Production Actually Requires
Let’s get specific about what your skin needs to build and maintain collagen – because this is where the internal work you’ve already done becomes your biggest asset.
Amino acids – particularly glycine, proline, and hydroxyproline.
Collagen is a protein. Specifically, it’s a triple-helix structure made primarily of glycine, proline, and hydroxyproline. Without adequate dietary protein and the specific amino acids that compose collagen, your body simply cannot build it – regardless of what you apply topically or what treatments you undergo.
Vitamin C.
Vitamin C is a required cofactor for collagen synthesis. It’s essential for the hydroxylation of proline and lysine – the step that stabilizes the collagen triple helix. Without it, collagen production stalls even when amino acids are available.
Copper and zinc.
These trace minerals are required for collagen cross-linking – the process that gives collagen its structural strength and elasticity. Deficiency in either leads to weaker, less resilient collagen fibers.
Retinol (Vitamin A).
Vitamin A directly stimulates fibroblast activity – the cells responsible for producing collagen. It also regulates skin cell turnover and supports the structural integrity of the dermis.
Hormones – particularly estrogen and progesterone.
Estrogen receptors are present throughout the skin. Estrogen directly stimulates collagen synthesis and maintains skin thickness, hydration, and elasticity. This is why skin changes so dramatically during perimenopause – and why hormonal balance is a non-negotiable part of the skin aging conversation.
Circulation.
Collagen-building fibroblasts need oxygen and nutrients delivered via blood flow. Poor circulation means the building blocks are available but can’t reach the cells that need them.
Light signaling.
Specific wavelengths of light – particularly near-infrared and red light – directly stimulate mitochondrial activity in skin cells, increase ATP production, and activate fibroblasts. This is not a fringe concept. It is one of the most well-researched mechanisms in photobiomodulation science.
External support
If you’ve been eating intentionally, supporting your hormones, and reducing inflammation… you have already built the most important foundation for collagen production that exists. Now the question is: what are you doing externally that matches that foundation?
Explore the Nira Pro 3 Laser – code STEAGUE10 →
The Problem With Cycling Through Damage
Here’s what I’ve observed – in my own journey and in the women I work with: the damage-based treatment cycle is seductive because it produces visible results. You do the treatment. You see improvement. You feel like something is working.
But then it fades. And you go back. And each time, you need the treatment to maintain what you’ve built – because the treatment isn’t teaching your skin to produce collagen on its own. It’s triggering a repair response that requires the original injury to sustain itself.
Meanwhile: your skin barrier takes repeated hits, inflammation accumulates over time, for autoimmune women each treatment is a potential immune trigger, the results become harder to maintain and easier to lose.
This is the cycle. And most women don’t realize they’re in it until they’ve been doing it for years.
A Different Question to Ask
What if instead of asking “how do I trigger my skin to repair?” you asked: “how do I support the repair my skin is already trying to do?”
That reframe changes everything. Because your body – especially after the internal work you’ve done – is already oriented toward repair. It’s already trying to build collagen, regulate inflammation, and maintain structural integrity. It doesn’t need to be forced through damage to get there. It needs the right signal.
What I’ve Been Testing (and Why It Makes Sense to Me)
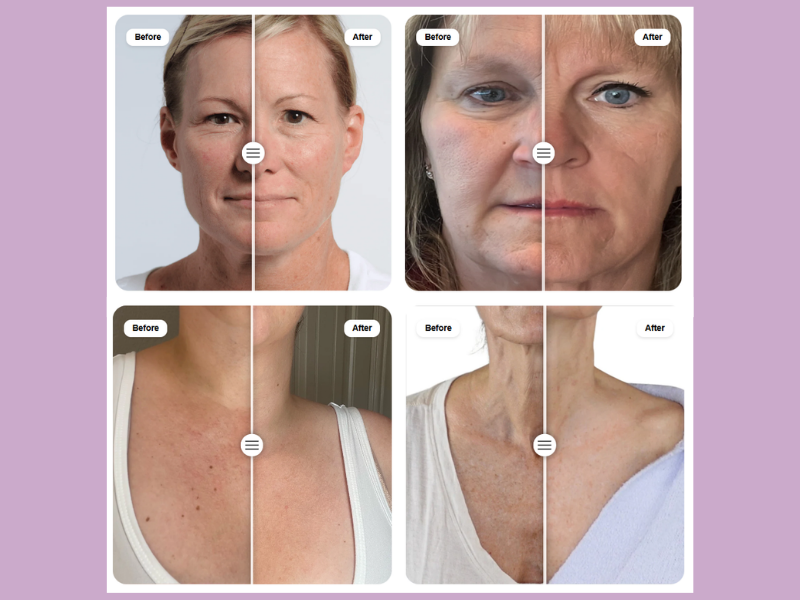
I’ve been using the Nira Pro 3 – a clinical-grade laser device designed for at-home use that stimulates collagen production through non-ablative laser energy.
Non-ablative means: no damage to the skin surface. Instead of injuring tissue to trigger repair, it delivers energy at a wavelength that penetrates into the dermis and directly stimulates fibroblast activity – the cells that produce collagen.
No downtime. No inflammation. No barrier disruption. No immune trigger. Just a direct signal to the cells that build collagen, telling them to do more of what they’re already designed to do.
For me, this is the external approach that finally aligns with everything else I’m doing internally. I’m not forcing my skin through stress to get results. I’m supporting the process my body is already running. That coherence matters to me. And I think it will matter to you too.

Nira Pro 3 Laser – use code STEAGUE10 for your discount
What This Looks Like Over Time
This is not a one-treatment result. And I want to be honest about that. Collagen remodeling is a slow process – because collagen itself has a long turnover cycle. Real, structural improvement in skin firmness, texture, and elasticity takes consistent support over weeks and months.
But here’s the difference: when you’re building collagen through biological support rather than damage cycles, the results are cumulative – they build on each other rather than fading between treatments; sustainable – because you’re strengthening the underlying structure, not just triggering temporary repair; aligned – with everything else you’re doing internally, so your whole system is moving in the same direction.
This is what aging well actually looks like. Not chasing treatments. Not maintaining damage. Building, consistently, from the inside out and the outside in.
The Full Picture
I want to zoom out for a moment. Because this post is really about something bigger than a laser device. It’s about coherence.
And you deserve an external approach that honors it. Not one that works against your biology. Not one that requires repeated damage to maintain. Not one that treats your skin like a problem to be managed.
One that says: your body already knows how to do this. Let’s give it what it needs to do it better.
That’s beauty biology. That’s what this whole series has been about. And that’s what you’ve been building toward – whether you knew it or not.
Explore the Nira Pro 3 Laser – code STEAGUE10 →

What has made the biggest difference in your skin so far?
Internal work, external treatments, or both? I’d love to hear where you are in this journey. Drop it in the comments.

References
Varani J et al. Decreased collagen production in chronologically aged skin: roles of age-dependent alteration in fibroblast function and defective mechanical stimulation. Am J Pathol. 2006;168(6):1861–1868.
Proksch E et al. Oral supplementation of specific collagen peptides has beneficial effects on human skin physiology: a double-blind, placebo-controlled study. Skin Pharmacol Physiol. 2014;27(1):47–55.
Avci P et al. Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring. Semin Cutan Med Surg. 2013;32(1):41–52.
Fisher GJ et al. Mechanisms of photoaged skin: a review of the role of matrix metalloproteinases. Arch Dermatol. 2002;138(11):1462–1470.
Shah MG, Maibach HI. Estrogen and skin: an overview. Am J Clin Dermatol. 2001;2(3):143–150.

